

FemoroAcetabularImpingementApp
Femoroacetabular impingement (FAI) is a recognized cause of hip pain in the young adult and is postulated to be a major cause of early osteoarthritis. Femoroacetabular impingement is a mismatch between the shape of the head–neck junction and the acetabulum. Hump malformation of the femoral head-neck junction (Cam) or femoral head acetabular over-coverage (pincer) leads to a damage to the articular cartilage and arthritis. The best radiological means of measuring FAI is CT scan or MRI, however, due to substantive radiation dose in CT and high cost in MRI, there are not routinely used in clinical practice for examinations. Femoral head/neck asphericity is best detected with the Dunn-projection-view in 45°, projection that is not always available. FAI is detectable also to an acceptable and conclusive level on standardised common AP pelvic radiographs.
The app is medical software aimed for orthopaedic surgeons, providing tools that allow doctors to:
-Securely import medical images directly from the camera or stored photos.
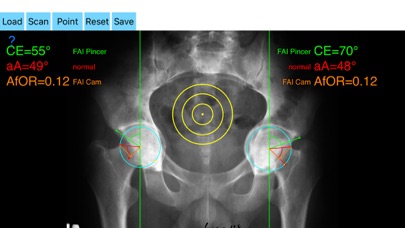
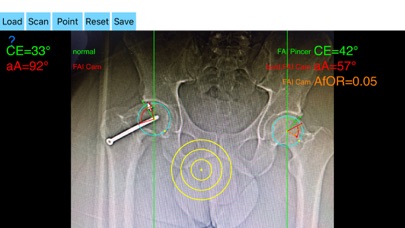
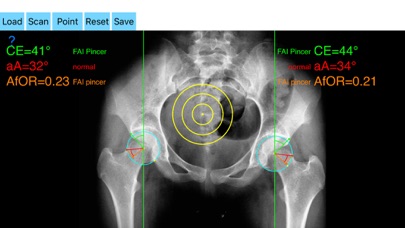
Offers a very convenient way to determine the most accurate possibly lines in order to measure the angles. By the aid of a circular transparent template, the points of interest are marked accurately. The circular template help to detect and mark easily, the alpha point - where the radius of the curvature of the femoral head first exits the circle of best fit corresponding to a circular head - real turning point of asphericity of femoral head
The drawn lines between points, allows app to estimate in radiographs, Center-Edge Angle (CE), α - angle (aA) and the anterior femoral offset ratio (AfOR). The measured values are compared with values from normal reference database. In case the measured angles are beyond the normal range, the hip is categorized as normal, dysplastic, borderline dysplastic hip and the type of femoroacetabular impingement (FAI) deformity namely cam type, pincer type or mixed is printed over the screen accordingly. Measures by the app are not affected by the X-ray projection.
-Save the planned images, for later review or consultation.
Disclaimer.
Regarding its plausibility app offers no diagnosis or treatment. App provide an early indication that further evaluation may be warranted by Speciality Doctor. Explicitly is announced that the apps are not for diagnosis. Clinical judgment and experience are required to properly use the software. App alone do not replace an M.D. or specialist. All information received from the App output must be reviewed before any attempted treatment. The software is not for primary image interpretation. Any influence to the operators in making decisions remains user own responsibility and experience. App does not dispense medical advice. Patient should seek a doctor’s advice in addition using the app and /or before making any medical decisions for themself. Never substitute or replace doctors advice or change treatment modalities based on any measured outcome. App indicated for assisting healthcare professionals for scientific and research reason. Clinical judgment and experience are required to properly use the app and further research and validation is pending in coming future.
The app is a handy tool for an orthopaedic surgeon, radiologist, medical student or resident who wants objectively to monitor and determine femoroacetabular impingement (FAI) of the hip. The build-in comparison feature with the normal reference values and the combination of angles may help decide what could be considered normal or cam and or pincer type of FAI. The app is not a simple goniometer, is an enhanced product.This is particular useful especially in clinical settings where you need a quick results without losing time in looking for reference data and in doubtful cases.